
If you’ve ever taken an antidepressant, antipsychotic, or certain mood stabilizers, you may have heard your doctor mention something about “QTc” or “heart rhythm.” Most people nod, take the prescription, and move on — but behind that casual warning lies one of the most serious (though thankfully rare) side effects of many psychotropic medications: QTc interval prolongation and the life-threatening arrhythmia called Torsade de Pointes.
A detailed review in Deutsches Ärzteblatt (updated in recent years) dives deep into this topic, highlighting which drugs carry the highest risk, why it happens, who is most vulnerable, and — most importantly — how doctors and patients can minimize the danger without giving up effective psychiatric treatment.
Also Read


This isn’t just theoretical. Real patients have died or suffered cardiac arrest from this side effect. Understanding it can literally be a matter of life and death — especially for people on multiple medications or with other heart risk factors.
What Exactly Is the QTc Interval?
The QT interval is a segment on an electrocardiogram (ECG) that measures the time it takes for the heart’s ventricles to electrically depolarize and repolarize — in simple terms, the time from when the heart starts a beat until it’s ready for the next one.
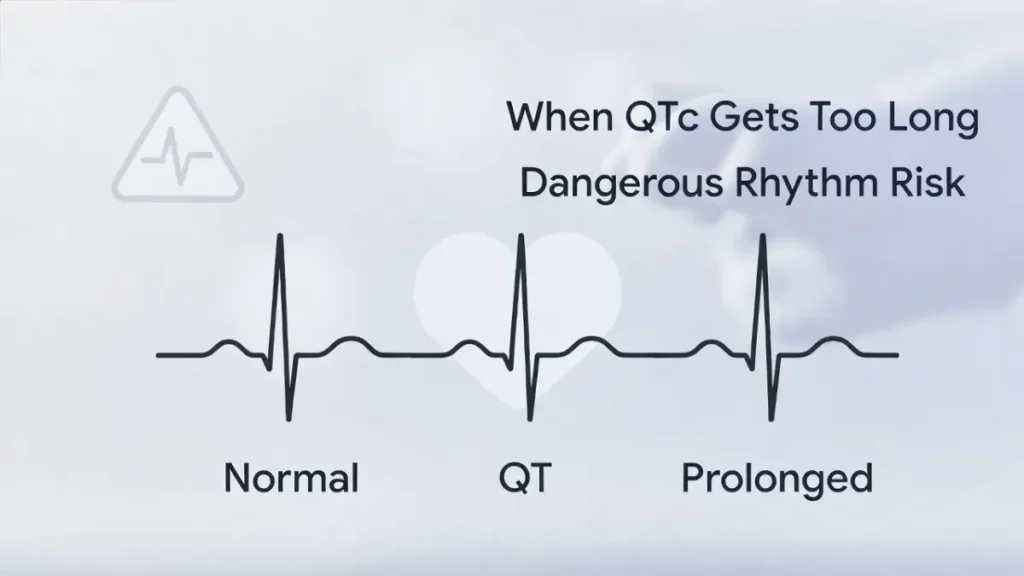
Because heart rate affects this interval, we correct it for rate: that’s QTc (corrected QT). Normal QTc values are:
- Men: <430–450 ms (depending on guideline)
- Women: <450–470 ms
- Prolonged QTc: generally >450 ms (men) or >470 ms (women)
- Very high risk: >500 ms or an increase of >60 ms from baseline
When QTc gets too long, the heart becomes electrically unstable. Early afterdepolarizations can trigger a dangerous polymorphic ventricular tachycardia called Torsade de Pointes (“twisting of the points” on ECG) — which can degenerate into ventricular fibrillation and sudden cardiac death.
Which Psychotropic Drugs Are the Biggest Offenders?
Not all psychiatric medications carry the same risk. The Ärzteblatt review and international databases (CredibleMeds, Arizona CERT) classify them into categories:
High / Known Risk of Torsade de Pointes (avoid if possible in patients with QTc risk factors):
- Thioridazine (Melleril) — historically the worst offender
- Ziprasidone (Zeldox/Geodon)
- Intravenous haloperidol (especially high doses)
- Pimozide
- IV droperidol (less common now)
Conditional / Moderate Risk (risk increases with dose, combinations, or other factors):
- Citalopram (especially >40 mg/day)
- Escitalopram (risk lower than citalopram but still present)
- Quetiapine (Seroquel)
- Chlorpromazine
- Amisulpride
- Methadone (used in opioid maintenance, but relevant in psychiatry)
- Some tricyclic antidepressants (e.g., amitriptyline, clomipramine) at high doses
Low / Minimal Risk (generally safe regarding QTc):
- Sertraline
- Fluoxetine
- Paroxetine
- Mirtazapine
- Bupropion
- Most benzodiazepines
- Lamotrigine, valproate, lithium (lithium can cause bradycardia but not direct QT prolongation)
Special Note on SSRIs: Citalopram and escitalopram received FDA and EMA warnings in 2011–2012. Maximum recommended doses were lowered (citalopram 40 mg/day in adults, 20 mg in >60 years or liver impairment). Escitalopram is safer than citalopram at equivalent doses but not risk-free.
Why Do These Drugs Prolong QTc?
Most psychotropics that affect QTc block the rapid delayed rectifier potassium current (IKr) in cardiac cells — specifically the hERG potassium channel. This prolongs the repolarization phase, setting the stage for early afterdepolarizations.
Risk multiplies when several factors combine:
- High dose
- Female sex (women have longer baseline QTc)
- Older age (>65)
- Hypokalemia or hypomagnesemia
- Bradycardia
- Congenital long QT syndrome
- Other QT-prolonging drugs (antibiotics like erythromycin, antifungals like fluconazole, antiarrhythmics like amiodarone)
- Heart disease or electrolyte disturbances
The most dangerous scenario: a patient on citalopram + quetiapine + ondansetron (anti-nausea drug) + low potassium after vomiting.
How Big Is the Real-World Risk?
Torsade de Pointes is rare — even with high-risk drugs. Estimates range from 1:1000 to 1:100,000 treated patients, depending on the drug and patient factors.
But because millions take these medications, even a tiny risk translates to real cases of sudden death or resuscitated cardiac arrest — often in people who seemed perfectly healthy otherwise.
Practical Safety Rules Doctors (and Patients) Should Follow
- Baseline ECG — Recommended before starting high-risk drugs (ziprasidone, IV haloperidol, thioridazine, high-dose citalopram) and in patients with known heart disease or multiple risk factors.
- Repeat ECG — If dose increases significantly, new symptoms (palpitations, syncope), or adding another QT-prolonging drug.
- Stop or reduce if QTc >500 ms or increases >60 ms from baseline.
- Correct electrolytes — Keep potassium >4.0 mmol/L and magnesium >0.8 mmol/L.
- Avoid unnecessary combinations — Check every new drug with tools like CredibleMeds.org or the Arizona CERT list.
- Patient education — Warn about symptoms of arrhythmia: sudden dizziness, palpitations, fainting.
Bottom Line: Treatment vs. Safety Balance
Psychotropic drugs save lives every day — treating severe depression, psychosis, bipolar disorder, and anxiety. The QTc risk, while real, is manageable in most cases with awareness, baseline checks, careful dosing, and avoiding dangerous combinations.
The key message from the Ärzteblatt review is clear: We don’t need to panic and stop effective treatment — but we do need to be vigilant.
If you’re on citalopram, quetiapine, ziprasidone, or any psychiatric medication and you have heart concerns, a family history of sudden death, or are taking other QT-risk drugs, talk to your psychiatrist and ask about an ECG. A simple 30-second test can provide peace of mind.
Have you ever had a doctor mention QTc prolongation when prescribing a psychiatric medication? Or has anyone in your circle experienced heart rhythm issues while on these drugs? Real experiences help make this topic less abstract — feel free to share below.





 Important Notice -The content on this website is provided for general informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health-related decisions.
Important Notice -The content on this website is provided for general informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health-related decisions.